Residency Curriculum Enhancement: A Fundamental Education Tool to Improve Antibiotic Prescribing
Introduction
The Accreditation Council for Graduate Medical Education (ACGME) requires that family medicine residents demonstrate competency in patient care including, but not limited to, ability to use pharmacotherapy.1 While our current curriculum in family medicine includes inpatient pharmacist teaching throughout the required six blocks of medicine, we identified a gap in foundational knowledge necessary to safely prescribe antimicrobial therapy in inpatient settings.
Background
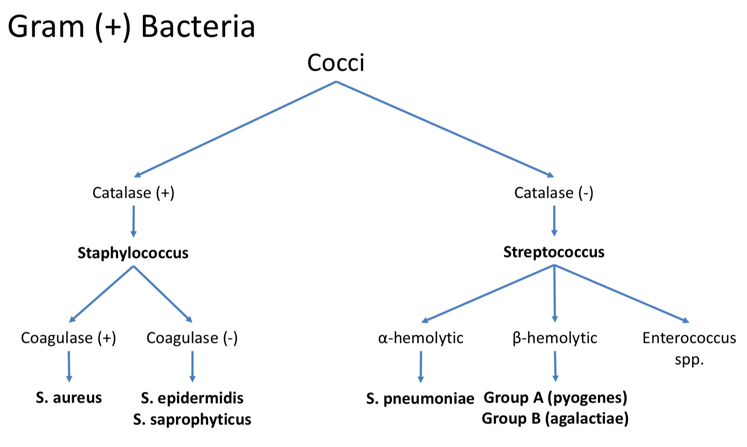
Proper antibiotic selection for suspected infection must be taught and reinforced for a family medicine resident to be successful during training and future practice. The American Society of Health-System Pharmacists (ASHP) identifies antimicrobial stewardship and promoting the optimal use of antimicrobial agents as part of the pharmacist’s role, which our program enables by having a clinical pharmacist on faculty to educate both resident and faculty prescribers.2 As our family medicine residency aimed to improve our curriculum for the inpatient medicine rotation at our midsized community hospital, we identified that isolated discussion of infectious disease cases as they arose on the inpatient service did not adequately convey the fundamental knowledge required to connect the guideline-recommended drug to the suspected infectious disease. Therefore, a lecture incorporating the basic science of microbiology and antimicrobials, ie, “bugs and drugs,” was developed to foster rational prescribing habits regarding empiric antibiotic selection. This small study was undertaken to assess the residents’ perceived preparedness, before and after the lecture, to prescribe empiric antibiotics for a suspected infection.
Methods
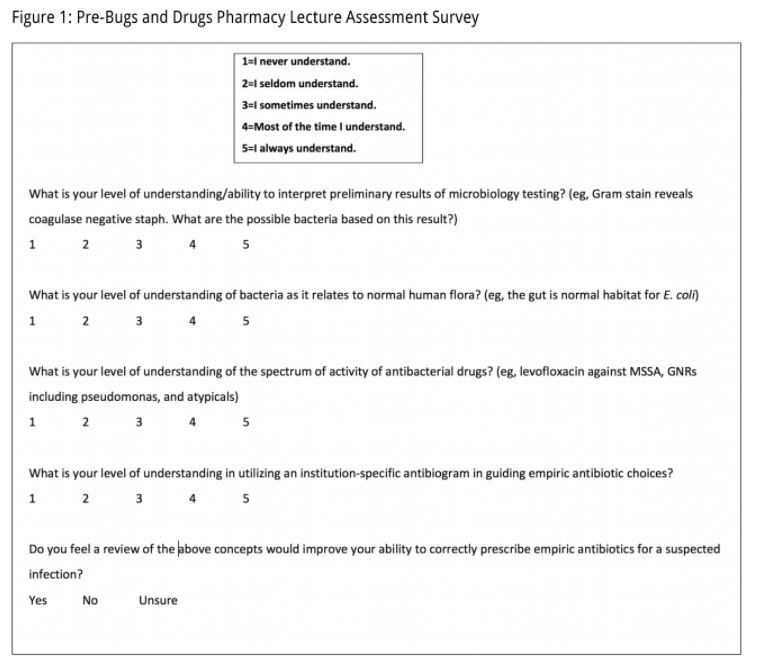
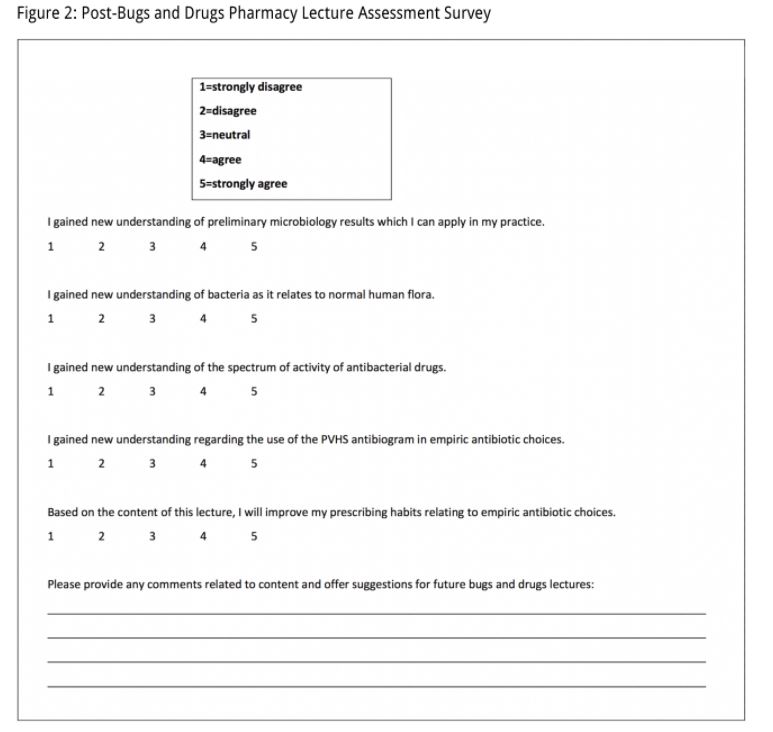
Our institutional review board approved this study. The family medicine faculty pharmacist developed and delivered a 1.5-hour “bugs and drugs” lecture, which incorporated active learning, to each postgraduate year one (PGY-1) medicine resident during their inpatient medicine rotation. A six-page lecture outline, with objectives, was provided to each resident intern for taking notes and utilization as a reference/resource during the medicine rotation. A survey administered prior to the lecture (Figure 1) assessed current, individual level of understanding of specific content areas (Table 1). The second survey, administered after the lecture (Figure 2), assessed perceived preparedness to rationally prescribe empiric antibiotics after the “bugs and drugs” education. The pre- and postlecture surveys were administered anonymously on the same day as the lecture.
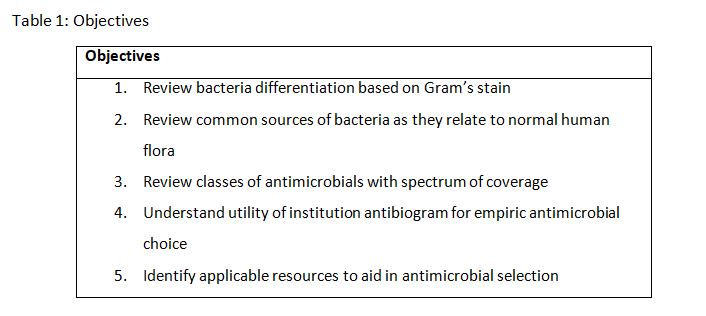
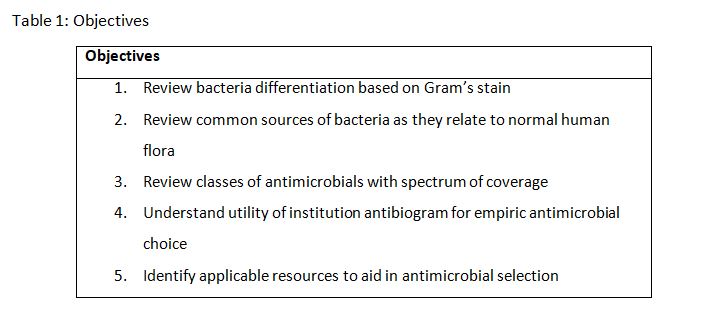
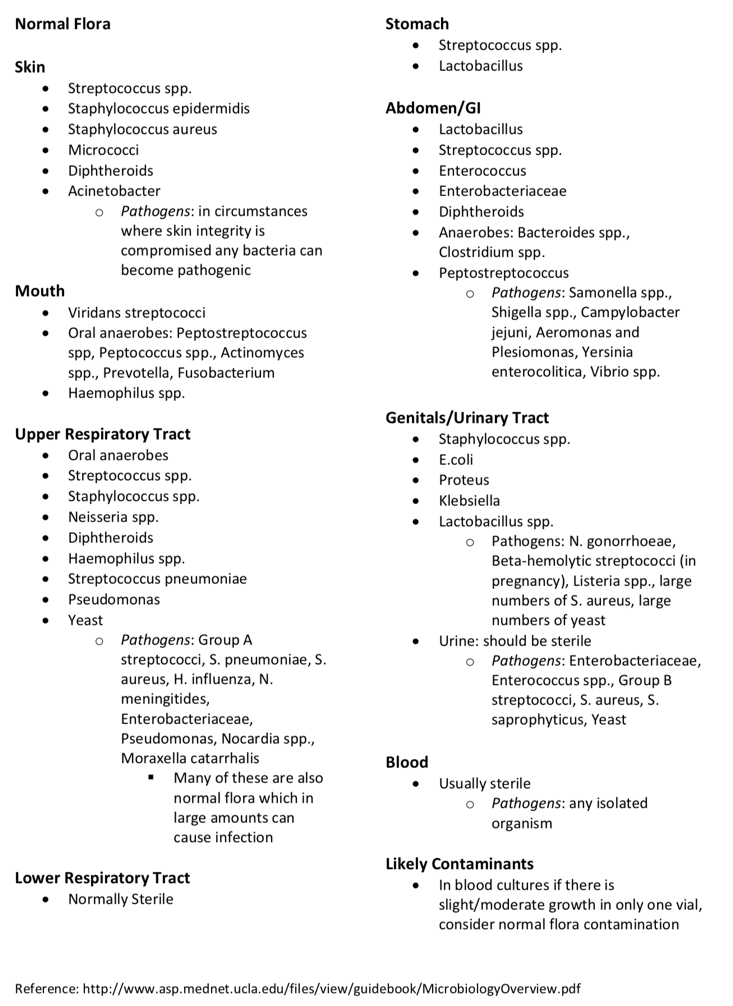
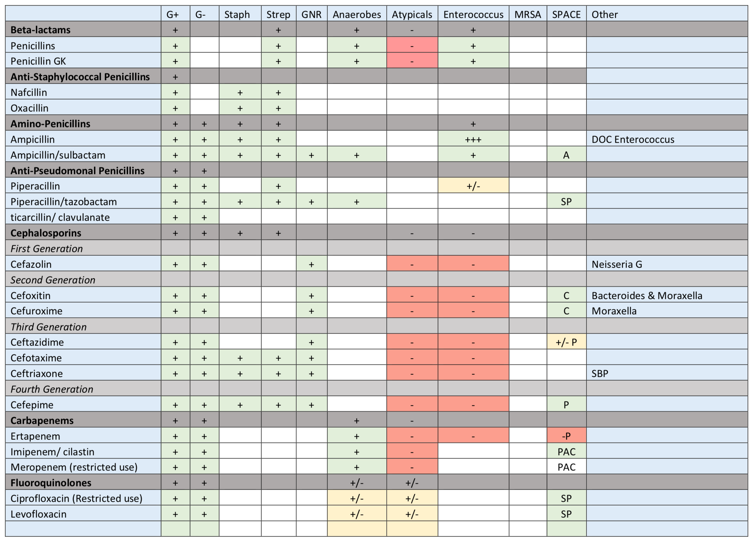
Exercises were designed to incorporate use of the institution’s antibiogram throughout the lecture, allowing residents to demonstrate their ability to choose appropriate agents for the community, including the most drug-resistant organisms such as pseudomonas, s. pneumoniae, and methicillin resistant staphylococcus aureus.
Results
A total of 12 residents participated in the learning activity and completed both surveys. Ninety six percent of residents surveyed believed receiving a “bugs and drugs” lecture improved their preparedness to rationally prescribe empiric antibiotics for a suspected infection. Although additional statistical evaluation is not suitable for such a small sample, this suggests an increase in the perception of resident preparedness to prescribe rational empiric antibiotics for a suspected infection as a consequence of this didactic session. While all questions on each of the surveys were answered, few additional comments were provided, as requested at the end of each pre- and postsurvey. When postlecture survey results were assessed in this individual PGY, an area of concern was understanding bacteria as they relate to the source of infection.
Discussion
Overall, our project has led to a culture change on the medicine service. The initial intent was designed to improve knowledge around an important focused topic, and it has created a framework for reinforcing the topics, using just-in-time resources to aid in clinical decision-making. Beyond that, it has encouraged residents to request more formalized teaching on the inpatient medicine rotation in general. The results of this study have led to the lecture being delivered during each intern’s first week on the medicine rotation, and within their first 6 months of residency. In addition, each PGY-2 and PGY-3 on the service will have received the lecture several times as well, by the time they graduate. Since implementation of this bugs and drugs lecture, residents refer to lecture notes to aid in rational empiric antibiotic selection across the continuum of residency. While the lecture is delivered using a dry erase board with residents taking notes, an electronic version of the core content is posted for reference on the family medicine residency’s wiki (attached).
Conclusion
Adopting a systematic, step-wise approach to teaching and learning antibiotics assists in rational and logical antibiotic prescribing. Other residencies could explore similar interventions by first assessing their current approaches to teaching antibiotic prescribing. This should include identification and characterization of resources already in use by residents. We believe our intervention benefited from using formatting and organization similar to popular tools.
Residencies without formal antibiotic teaching are ideally suited to collect and analyze before and after data; such data could include observations of antibiotic selection and management discussions during rounds, or chart review of resident notes. Collecting these data in addition to survey data will add to the overall quality of evidence supporting this kind of educational intervention.
References
1. Accreditation Council for Graduate Medical Education. ACGME Program Requirements for Graduate Education in Family Medicine. Effective July 1, 2017. https://www.acgme.org/Portals/0/PFAssets/ProgramRequirements/120_family_medicine_2017-07-01.pdf. Accessed April 25, 2018.
2. ASHP statement on the pharmacist’s role in antimicrobial stewardship and infection prevention and control. Am J Health Syst Pharm. 2010; 67(7):575–577. https://doi.org/10.2146/sp100001.
Attachments